

Abstract
Acute myeloid leukemia (AML) is a devastating disease; however 20%-30% of patients will achieve long term remission. The long-term follow up of AML patients who received bone marrow transplantation (BMT) is well documented. It remains unclear though whether AML long-term survivors who did not undergo BMT (LTSnoBMT) return to normal health. In order to answer this question a large cohort of AML patients and well matched controls are needed. For the present study, the electronic health records (EHR) of 4.2 million individuals covering over 16 years of follow up were studied. Morbidity and mortality of LTSnoBMT were compared to a large number of age-matched controls.
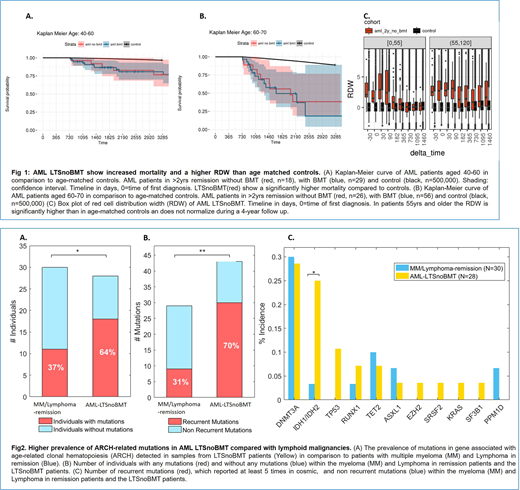
We identified 177 LTS who were in remission two years after AML diagnosis of which 61 were LTSnoBMT. The mortality of LTSnoBMT 10 years after diagnosis was 20%-50% higher in comparison to controls in an age dependent manner with higher mortality among the elderly LTS (Figure 1A, B). While several lab results were different between the LTSnoBMT and controls, most strikingly the red cell distribution width (RDW) of the LTSnoBMT was much higher among elderly LTSnoBMT (Figure 1C). High RDW has been previously reported to correlate with mortality. Recent studies found that high RDW predict AML and even greater correlation of high RDW with mortality among individuals carrying age related clonal hematopoiesis (ARCH) mutations was detected.
To investigate the genetic profile of LTSnoBMT, a deep-targeted sequencing method (covering 32 recurrently mutated genes in AML) was used. Remission samples (at least 2 years from diagnosis) from 28 LTSnoBMT were analyzed. In most cases mutations which were detected at diagnosis, were not present in the remission samples. ARCH defining events (most of them new) were found in 64% of the LTSnoBMT. To evaluate whether this high prevalence of ARCH related mutations among LTSnoBMT patients is related to chemotherapy exposure, we also studied 30 individuals with lymphoid malignancies who received chemotherapy and were in remission. The prevalence of ARCH related mutations in the controls was significantly lower (37%) than in the LTSnoBMT (Figure 2A) (p=0.035). Higher prevalence of IDH1/2 mutations was found among LTSnoBMT (Figure 2C) (p=0.017). Furthermore, 70% of the mutations detected in the LTSnoBMT were recurrent (i.e. has more than 5 occurrences in COSMIC data base) compared to 31% in the controls (Figure 2B) (p=0.001).
Altogether, AML is a complex disease where even after the sustainable eradication of the malignant clone, the hematopoietic system/microenvironment does not normalize. The reported correlation between ARCH and mortality suggests that the high prevalence of ARCH related mutations among LTS might contribute to the high mortality that we observed. Our findings have both biological and clinical implications. Future studies should determine the reasons why AML - LTS have such high prevalence of ARCH with specific mutations and increased mortality. Furthermore, closer clinical follow up including mutation analysis should be considered for these individuals.
Cilloni:Celgene: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees. Metzeler:Celgene: Consultancy, Research Funding; Novartis: Consultancy. Ofran:Novartis: Other: Served on a Novartis advisory board.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal